What is PAH?
PAH Is a Rare, Serious, and Progressive Disease1
- PAH results from restricted flow through the pulmonary arteries, leading to increased pulmonary vascular resistance (PVR)2
- Increased PVR leads to a decline in RV function and eventual RV failure2
Hemodynamic definitions of PH and PAH1
The definitions are based on hemodynamic assessment by an RHC
PH
mPAP >20 mmHg
PAH
mPAP >20 mmHg PAWP ≤15 mmHg PVR >2 WU
PAH symptoms may present like other lung conditions3,4
- While a majority of patients present with dyspnea on exertion, it is important to distinguish PAH from other cardiac or pulmonary etiologies such as asthma or COPD
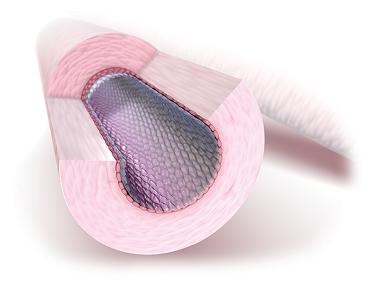
Increased PVR is caused by narrowing of the pulmonary arteries2
Increased PVR leads to a decline in RV function and eventual RV failure.2
Hemodynamic changes correlate with increasing severity of PAH5
Peak cardiac output
Resting cardiac output
Resting PAP
PVR

Time
Peak cardiac output
Resting cardiac output
Resting PAP
PVR

Normal PVR:
≤2 Wood units.1
Elevated PVR:
>2 Wood units.1
Adapted from Eur Respir Rev.
2011;20(122):236-242.
Time
Common signs and symptoms of PAH in the REVEAL Registry3*†

*Percentages are approximations.

PAH is associated with diverse pathologic events
Pulmonary vasoconstriction
The pulmonary arteries contract, and vascular resistance increases.5,6
Right ventricular strain and dysfunction
Chronic elevated pressures lead to right ventricular strain and overload.5,7
Fibrosis
Over time, the vascular intima thickens, further impeding blood flow.7
Hypertrophy
Vascular hypertrophy occurs in the presence of developing lesions and other arterial abnormalities.7,8
In situ thrombosis
Abnormalities in platelet activation and function promote thrombosis and can lead to increased vasoconstriction.8
PAH Pathways
There are 4 pathways in PAH with specific drug classes1,9
PAH involves an imbalance of naturally occurring chemicals in the body (endothelin, prostacyclin, and nitric oxide), as well as dysregulation of the activin signaling pathway, all of which contribute to changes in the blood vessels.
Nitric Oxide Pathway1,10
PDE5i, sGCs promote
- Anti-proliferation
- Vasodilation
Endothelin Pathway1,11
ERAs prevent
- Vasoconstriction
- Cellular proliferation
Prostacyclin Pathway1,10,12
Prostacyclin pathway agents promote
- Vasodilation
- Anti-proliferation
- Anti-inflammation
- Anti-thrombosis
Activin Signaling Pathway9
Activin signaling inhibitors prevent
- Cellular proliferation
- Inflammation
2022 ESC/ERS Guidelines: Focusing on multiple pathways is an effective treatment strategy with clinical benefits1